Breast reconstruction includes both partial and whole breast reconstruction
Oncoplasty includes adding plastic surgery procedures to
breast cancer surgery, to allow for a better breast shape, better placement of scars and offer breast conserving surgery to women with larger tumours or needing
larger / wider excision
due to tumour size or multiple tumours in the same area of the breast.
It can include partial breast reconstruction using various flaps or fat and skin from the area on the side of the breast or below the breast from the anterior abdominal wall or from the back.
Additionally in some oncoplastic procedures where appropriate, scars can be placed away from the tumor and be hidden near the areola or lower breast crease ( inframammary crease)
Is a surgical procedure performed to rebuild a woman's breast(s) after undergoing a mastectomy for breast cancer treatment.
It aims to restore the appearance of the breast, improve body image, and enhance the patient's quality of life. Breast reconstruction can be performed at the same time as the cancer surgery (immediate reconstruction) or after a delay (delayed reconstruction).
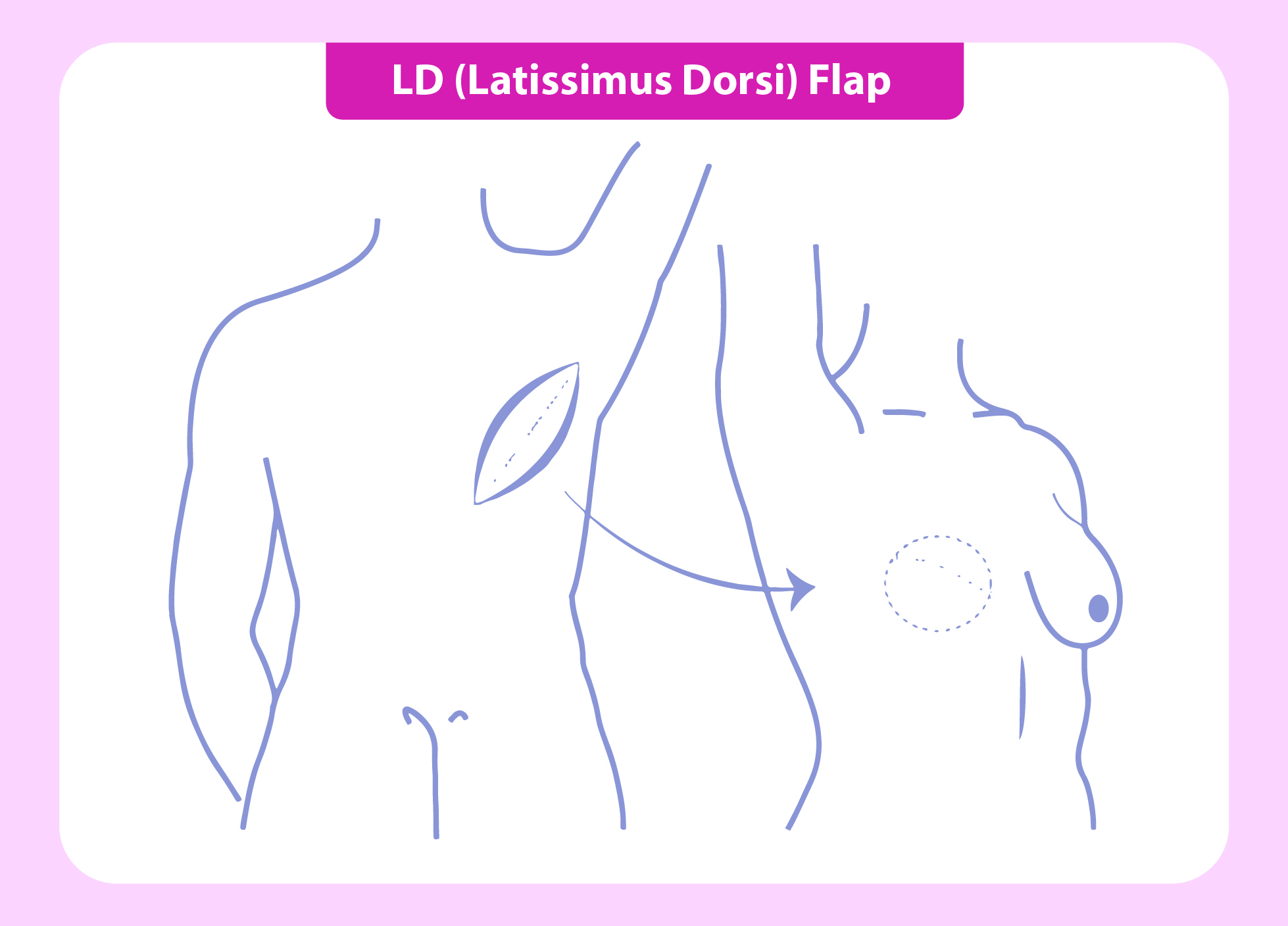
Perforator / Pedicled Flaps:
Perforator flaps are a specialized type of surgical technique used in breast reconstruction which involves the transfer of skin, fat,
and blood vessels from a donor site to reconstruct a specific area, such as the breast mound. Perforator
flaps are distinct from other flap-based procedures because they selectively preserve the perforating blood vessels.
Perforator flaps used for partial reconstruction include intercostal artey perforatory flaps, thoraco-epigastric perforator flaps.
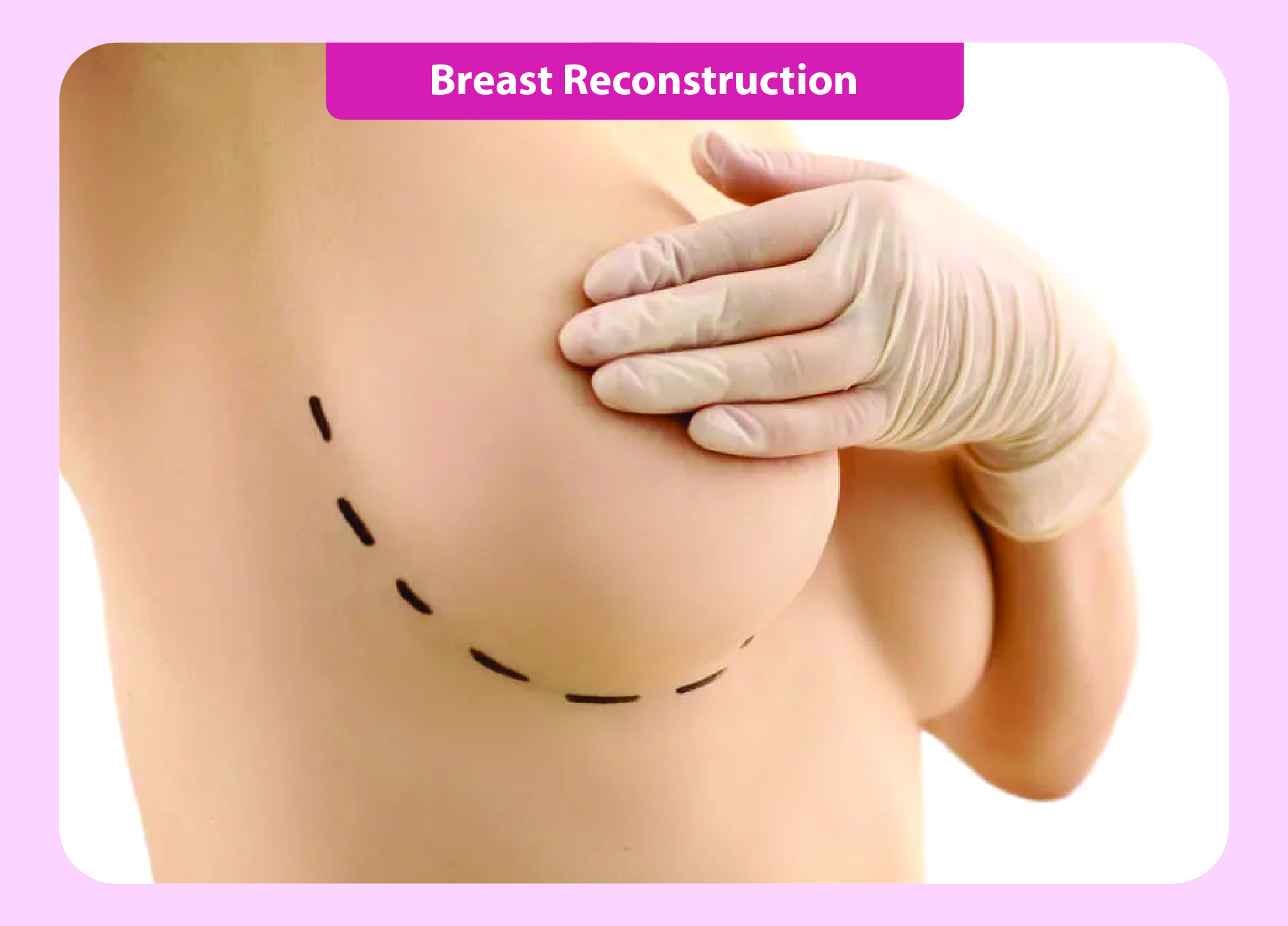
Pedicled flaps include the latissimus dosi flap. In this procedure, the surgeon utilizes the latissimus dorsi muscle, which is located
in the back, to transfer it along with skin and fat to the chest area to create the breast mound. The blood supply for the flap often
remains attached to the muscle, allowing it to be tunneled under the
skin to the chest. The LD flap can be used alone or in combination with implants to reconstruct the breast.
Whole breast reconstruction options included pedicled flaps like TRAM/ VRAM ( transverse or vertical rectus abdominus muscle flap) or microvascular free flaps using options mentioned below.
Deep Inferior Epigastric Perforator (DIEP) Flap: Utilizes skin and fat from the lower abdomen while sparing the abdominal muscle by preserving the perforating blood vessels from the deep inferior epigastric artery.
Superior Gluteal Artery Perforator (SGAP) Flap: Uses tissue from the upper buttock region while preserving the gluteal muscle by preserving the superior gluteal artery perforators.
Inferior Gluteal Artery Perforator (IGAP) Flap: Similar to SGAP, but uses tissue from the lower
buttock region by preserving the inferior gluteal artery perforators.
Silicone implants / expanders can also be an option offered for whole breast reconstruction.
This approach is particularly beneficial for women with larger breasts, ptotic breasts or tumors located in areas that could cause significant cosmetic deformity after a standard lumpectomy. The procedure involves the following steps:
The procedure involves the following steps:
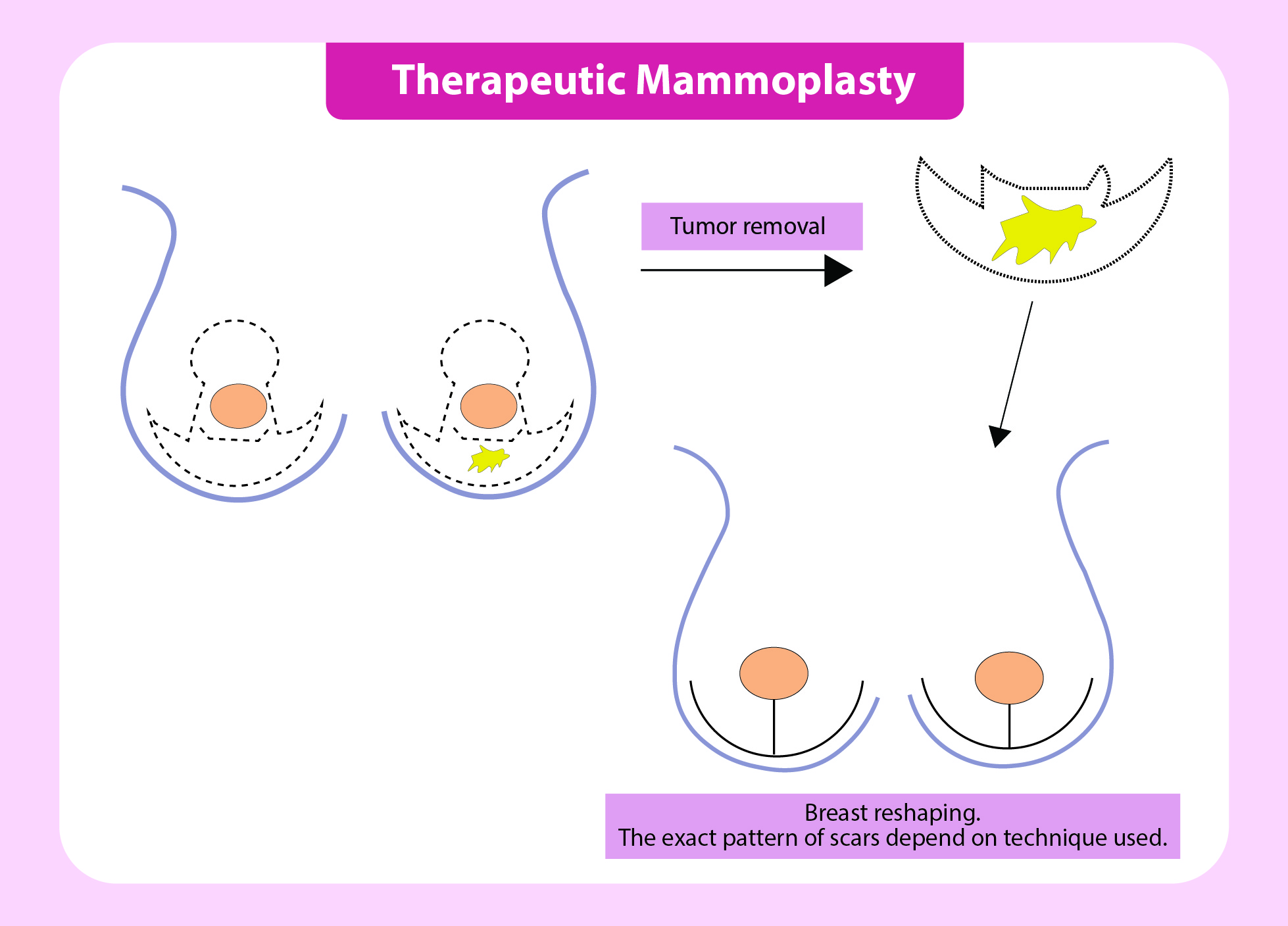
Tumor Removal: The surgeon removes the cancerous tumor and a surrounding margin of healthy tissue to ensure complete tumor removal (clear margins).
Breast Reshaping: After tumor removal, the breast is reshaped and contoured to achieve symmetry and an aesthetically pleasing appearance. The surgeon may rearrange the breast tissue or perform a breast reduction or lift to achieve the desired outcome.
Suturing: The incisions are closed using surgical sutures to secure the breast's new shape.
Improved Cosmetic Outcome: By incorporating plastic surgery techniques, therapeutic mammoplasty can lead to a more symmetrical and natural-looking breast appearance.
Psychological Benefits: Preserving the breast's appearance can have a positive impact on a woman's body image and self-esteem during and after cancer treatment.
Breast Conservation: Therapeutic mammoplasty allows for tumor removal while maintaining a significant portion of the breast tissue, avoiding the need for a complete mastectomy in some cases.
Single-Stage Procedure: In many cases, therapeutic mammoplasty can be performed in a single surgical procedure, reducing the overall treatment time.
Can breast reconstruction be done immediately after a mastectomy, or is it better to wait?
Reconstruction can be done immediately (during the same surgery as the mastectomy) or delayed until after other treatments like chemotherapy or radiation. The timing depends on your overall health, cancer stage, and personal preference. Your surgeon will guide you in making the best decision.
What are the risks and potential complications associated with breast reconstruction?
Common risks include infection, bleeding, implant rupture, scarring, or poor healing. Autologous reconstruction carries risks like hernia or muscle weakness at the donor site. Long-term issues may include implant displacement or changes in the reconstructed breast over time.
Will breast reconstruction affect my ability to detect breast cancer recurrence?
No, breast reconstruction does not interfere with cancer detection. However, regular follow-ups, imaging, and self-examinations remain important. Your oncologist and surgeon will recommend the appropriate monitoring plan.
What will the reconstructed breast look and feel like? Will it be symmetrical?
Reconstructed breasts can mimic the look and shape of natural breasts but may feel firmer or less sensitive. Achieving symmetry often involves additional procedures, such as adjusting the opposite breast. While results vary, advancements in techniques allow for highly natural outcomes.
How long does the recovery process take, and what restrictions will I have during recovery?
Recovery can take 4-8 weeks, depending on the procedure. You may need to avoid heavy lifting, strenuous activity, and specific arm movements. Follow-up visits will ensure proper healing, and your surgeon will give detailed post-surgery instructions.
Can I breastfeed with reconstructed breasts?
Breastfeeding is typically not possible with reconstructed breasts, especially if the breast tissue and milk ducts were removed during a mastectomy.
Does breast reconstruction require multiple surgeries?
Often, yes. The initial surgery is followed by additional procedures to refine the shape, reconstruct the nipple, or address complications, these can be spread over several months.
How does radiation therapy affect breast reconstruction outcomes?
Radiation can impact skin elasticity and healing, increasing the risk of complications like scarring or implant hardening. In such cases, autologous reconstruction may be a better option. Your surgeon will coordinate with your oncology team to plan accordingly.
What factors should I consider when choosing a surgeon for breast reconstruction?
Look for a board-certified plastic surgeon with experience in breast reconstruction. Request before-and-after photos, ask about patient outcomes, and read reviews. It’s also crucial to feel comfortable discussing your goals and concerns.
Can I exercise or return to work after breast reconstruction, and how soon?
Most light activities can resume after 4-6 weeks, but high-impact exercises or jobs involving heavy lifting may take longer. Discuss your recovery timeline with your surgeon.
What should I expect during my first consultation with a reconstruction surgeon?
During your consultation, the surgeon will review your medical history, discuss options, explain risks, and outline a surgical plan. Bring a list of questions and photos if you have specific aesthetic goals.